Endocarditis can happen at any age. Men are influenced about twice as regularly as ladies. IV medicate abusers and immunocompromised patients are at most noteworthy hazard.
Etiology
The ordinary heart is generally impervious to disease. Microbes and organisms don't effectively stick to the endocardial surface, and consistent blood stream keeps them from settling on endocardial structures. In this manner, 2 components are commonly required for endocarditis:
An inclining variation from the norm of the endocardium
Microorganisms in the circulation system (bacteremia)
Once in a while, gigantic bacteremia or especially destructive microorganisms cause endocarditis on typical valves.
Endocardial components
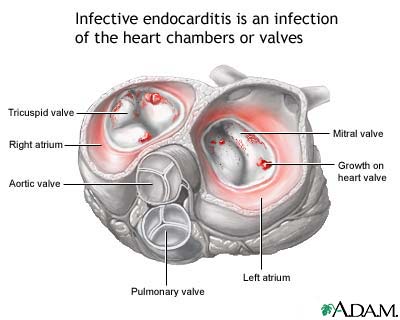
Endocarditis ordinarily includes the heart valves. Major inclining variables are innate heart surrenders, rheumatic valvular sickness, bicuspid or calcific aortic valves, mitral valve prolapse, hypertrophic cardiomyopathy, and earlier endocarditis. Prosthetic valves are a specific hazard. Periodically, painting thrombi, ventricular septal imperfections, and patent ductus arteriosus locales wind up noticeably contaminated. The genuine nidus for disease is generally a sterile fibrin-platelet vegetation framed when harmed endothelial cells discharge tissue figure.
Infective endocarditis happens regularly on the left side (eg, mitral or aortic valve). Around 10 to 20% of cases are correct sided (tricuspid or pulmonic valve). IV medicate abusers have a significantly higher frequency of right-sided endocarditis (around 30 to 70%).
Microorganisms
Microorganisms that contaminate the endocardium may begin from far off tainted destinations (eg, cutaneous canker, aggravated or tainted gums, UTI) or have evident entryways of passage, for example, a focal venous catheter or a medication infusion site. Any embedded remote material (eg, ventricular or peritoneal shunt, prosthetic gadget) is at danger of bacterial colonization, in this way turning into a wellspring of bacteremia and henceforth endocarditis. Endocarditis additionally may come about because of asymptomatic bacteremia, for example, commonly happens amid intrusive dental, restorative, or surgical methods. Notwithstanding toothbrushing and biting can bring about bacteremia (more often than not because of viridans streptococci) in patients with gingivitis.
Causative microorganisms change by site of disease, wellspring of bacteremia, and host hazard variables (eg, IV tranquilize manhandle), yet in general, streptococci and Staphylococcus aureus make 80 90% of cases. Enterococci, gram-negative bacilli, HACEK life forms (Haemophilus sp, Actinobacillus actinomycetemcomitans, Cardiobacterium hominis, Eikenella corrodens, and Kingella kingae), and growths cause the vast majority of the rest. Why streptococci and staphylococci oftentimes cling to vegetations and why gram-negative oxygen consuming bacilli at times follow are misty. Be that as it may, the capacity of S. aureus to cling to fibronectin may assume a part, as may dextran creation by viridans streptococci.
Subsequent to colonizing vegetations, microorganisms are secured by a layer of fibrin and platelets, which anticipates access by neutrophils, immunoglobulins, and supplement and therefore pieces have safeguards.
Pathophysiology
Endocarditis has neighborhood and systemic outcomes.
Neighborhood outcomes
Neighborhood outcomes incorporate arrangement of myocardial abscesses with tissue demolition and at times conduction framework anomalies (normally with low septal abscesses). Extreme valvular spewing forth may grow all of a sudden, bringing about heart disappointment and demise (typically because of mitral or aortic valve sores). Aortitis may come about because of bordering spread of contamination. Prosthetic valve contaminations are especially prone to include valve ring abscesses, impeding vegetations, myocardial abscesses, and mycotic aneurysms showed by valve deterrent, dehiscence, and conduction unsettling influences.
Systemic results
Systemic results are basically because of embolization of contaminated material from the heart valve and, principally in unending disease, resistant intervened wonders. Right-sided injuries ordinarily create septic aspiratory emboli, which may bring about aspiratory dead tissue, pneumonia, or empyema. Left-sided injuries may embolize to any tissue, especially the kidneys, spleen, and CNS. Mycotic aneurysms can frame in any significant supply route. Cutaneous and retinal emboli are normal. Diffuse glomerulonephritis may come about because of resistant complex statement.
Order
Infective endocarditis may have a slothful, subacute course or a more intense, fulminant course with more prominent potential for fast decompensation.
Subacute bacterial endocarditis (SBE), albeit forceful, for the most part grows deceptively and advances gradually (ie, over weeks to months). Regularly, no wellspring of contamination or entryway of passage is clear. SBE is brought about most usually by streptococci (particularly viridans, microaerophilic, anaerobic, and nonenterococcal amass D streptococci and enterococci) and less ordinarily by S. aureus, Staphylococcus epidermidis, Gemella morbillorum, Abiotrophia defectiva (some time ago, Streptococcus defectivus), Granulicatella sp, and critical Haemophilus sp. SBE frequently creates on unusual valves after asymptomatic bacteremia because of periodontal, GI, or GU contaminations.
Intense bacterial endocarditis (ABE) typically grows unexpectedly and advances quickly (ie, over days). A wellspring of disease or entryway of passage is regularly apparent. At the point when microscopic organisms are destructive or bacterial introduction is huge, ABE can influence typical valves. It is generally brought about by S. aureus, bunch A hemolytic streptococci, pneumococci, or gonococci.
Prosthetic valvular endocarditis (PVE) creates in 2 to 3% of patients inside 1 yr after valve substitution and in 0.5%/yr from that point. It is more typical after aortic than after mitral valve substitution and influences mechanical and bioprosthetic valves similarly. Early-onset diseases (< 2 mo after surgery) are brought on for the most part by pollution amid surgery with antimicrobial-safe microbes (eg, S. epidermidis, diphtheroids, coliform bacilli, Candida sp, Aspergillus sp). Late-onset diseases are brought on for the most part by sullying with low-harmfulness living beings amid surgery or by transient asymptomatic bacteremias, frequently with streptococci; S. epidermidis; diphtheroids; and the demanding gram-negative bacilli, Haemophilus sp, Actinobacillus actinomycetemcomitans, and Cardiobacterium hominis.
No comments:
Post a Comment